Since the age of 14, Sarah Reeves wanted to die. Respite from wishing herself dead came in short bursts. Once that respite came when she underwent electroconvulsive therapy, which sent massive electric shocks to her brain. But, the respite lasted only a few weeks. Nonetheless, she was encouraged by the outcome and went through the shock treatment again, only to see its effects wear off in weeks. She also tried transcranial magnetic stimulation, in which magnetic fields are used to stimulate nerve cells in the brain to improve symptoms of depression. Yet, the desire and desperation to die would come back to haunt her again and again.
At the age of 20, she was in a car crash with her brother Matthew. He recalls the first thing she told him after the crash: that she was so disappointed that she had not been killed. In her 30s, during a casual conversation, Sarah asked her mother if she knew what it was like to keep living when you really did not want to. Her mom said she did not know, but sought to know why Sarah had asked. To that, she said that she genuinely assumed that everyone would rather die than live. She did not realise such thoughts were unusual.
Sarah's depression “came on severely” at 14 and she tried “dozens and dozens of medications and therapies”, including cognitive and behavioural therapies, but none worked. When depression responds to medication, that might be enough to keep someone well for life. But, what Sarah had was treatment-resistant depression, in which the brain becomes resistant to medication and, sometimes, to other treatments as well. “No medication would stop me from wanting to kill myself,” Sarah, now 38, tells THE WEEK in an interview from Australia, along with Matthew.
If you ask her to pinpoint her triggers, she may not be able to. “I think that is what most people have difficulty understanding,” she says. “Because I have the most loving family and had a happy childhood. I never felt alone and I have really lovely friends as well. So there isn't something I could point to. I know there are lots of people who have had really hard lives and they do not have depression. So I think that depression is very much a physical disease―a disease of the brain. I can only say it is like cancer.”
She says that she worked hard with psychologists for more than two decades to try and change things, but in vain. “I had no symptoms; we first thought puberty could [have] been a trigger since it all started at 14, but then it stayed for so long,” she says, in a soft and assured voice―a sign that she was in complete control of her mind now.

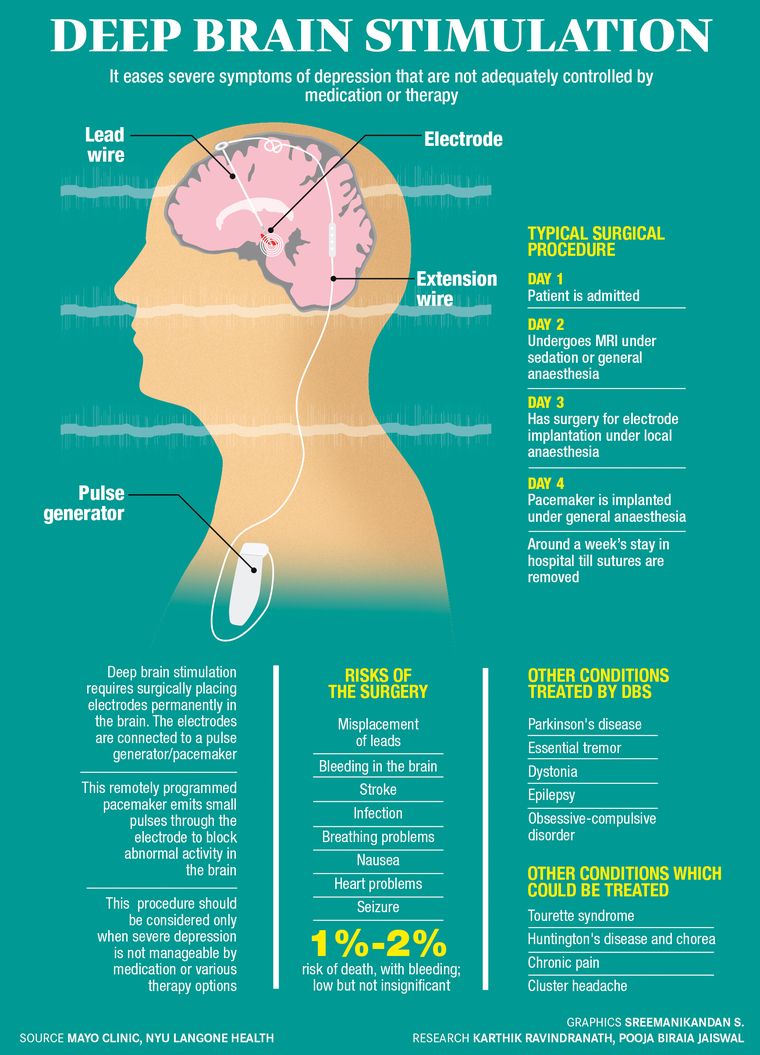
Around three months ago, Sarah underwent deep brain stimulation surgery for severe depression at Mumbai's Jaslok Hospital at the able hands of Dr Paresh Doshi, head of the department of neurosciences. DBS is mostly used for Parkinson's patients and it involves implanting electrodes in the brain under local anaesthesia. The electrodes are connected to a pacemaker through a subcutaneous wire. The pacemaker is programmed with a remote to emit small pulses of energy through the electrode to block abnormal activity in the brain.
“Before I heard about this surgery, I thought the end was coming,” says Sarah. When she came to India, she says, she had fully planned her suicide. “And, yeah, I was going to carry out that plan if [the surgery] did not help,” she says. “I had nothing to lose, I just felt really bad for my family. I did not expect it to work at all because I was just unable to believe that anything could help.”
 Safe hands: Dr Paresh Doshi, head of the department of neurosciences, Jaslok Hospital, Mumbai.
Safe hands: Dr Paresh Doshi, head of the department of neurosciences, Jaslok Hospital, Mumbai.
Now, she says that her energy is constantly increasing. “I am able to do more this week compared with last week,” she says. “So, I need to keep listening to my body to figure out when I need rest or when I can do more. I am in Sydney catching up with friends right now; something I have not had the energy for in a long time. I have been here one month and, at the start of my time here, I had to schedule a day between catch-ups to rest. But, in the weeks I have been here, I am not as tired after socialising anymore. So now I do not need much time between catch-ups.” She adds that she has met more friends than she had expected.
Post the surgery, she has started completing a monthly Montgomery-Asberg Depression Rating Scale. The scale determines the severity of depression. She says her scores are improving drastically. “My most recent score was almost three times [better] than my pre-surgery score,” she says. “So, in three months, my level of depression has more than halved, according to this scale.”
Matthew says psychologists diagnosed Sarah's depression to be organic, unlike the milder version of depression which can be treated with counselling and therapy. Organic depression does not seem to need any psychological trigger. “And it looks quite different,” says Matthew. “We noticed that Sarah's speech and her movements became slower. She had a lot less energy when her depression was bad and it had quite a physical impact on her.” They are a family of five, and Sarah's two brothers are married. Sarah, who is an occupational therapist, has not been able to work for five years and lives with her parents. “I have done various voluntary things, but not been able to properly work,” she says.
She says that with people like her, those who do not know them well do not see anything wrong. “I do not show it from the outside; you would not look at me and say she's planning her death,” she says. “But, it is quite common. That is why people are constantly shocked by celebrities or people who seem quite happy killing themselves. It is because it is a physical illness that someone can look quite normal, but they are not actually okay.” She laughs as she speaks, but the emotion is evident.

“Before surgery, I would just be in bed and then have a shower at 4pm or 5pm,” she says. “If I could, I would take my dog for a walk and then I would be so drained that I would need to get back to bed. So it was not just psychological or emotional, but a very physical lack of energy.” It was just very hard to do anything, she says, adding that it took her several hours to work up to having a shower, because that was so hard. “Sometimes, I [would] just sit on the bathroom floor, trying to make myself take a shower,” she says. “I used to wake up completely exhausted, like I had just run a marathon.”
Now, she says, she is just able to get out of bed and do things. “Just little things that I was not able to do, like housework, laundry, cooking, baking, making my parents tea,” she says. “I am able to go on really long walks. The other big difference has been wanting to spend time with people and actually having the capacity to do so. Earlier I would dread spending time with anyone, including my immediate family. It was not because I did not like them, just because my energy was so low and any interaction with humans was so draining.”
 Recovery tools: The black device around Sarah's neck charges her pacemaker.
Recovery tools: The black device around Sarah's neck charges her pacemaker.
Sarah has been regularly visiting Matthew and spending time with his kids. “Earlier, she would spent half an hour or one hour with my children and get too tired and leave,” says Matthew. “Now, she is more involved with them.” Most important, she is not having suicidal thoughts. “That is just a massive respite,” she says. “I do not know how to describe that, to not be thinking about death and not be in that constant state of despair.”
Doshi of Jaslok Hospital says that this lack of zest for life in people with organic depression is typically termed as anhedonia. He recalls the case of Benjamin, who was the first patient to have undergone the surgery for depression in Asia and Australia, in 2013. Doshi was his surgeon, too, and Sarah had also consulted Benjamin, a fellow Aussie. Ten years after surgery, Doshi says, Benjamin continues to improve and is now successful at his workplace. “He surfs and has children,” says Doshi. He adds that it usually takes six to eight months for patients to start getting the maximum benefit.
Sarah was anxious before the surgery because she felt it was her last option. Another issue was that she also had post traumatic stress disorder caused by a “couple of errors” during her shock treatment. She would have to be awake during the surgery and her head would be fixed into a frame and she would be bolted to avoid movement. “I knew that would definitely trigger my PTSD,” she says. “I prepared for it with my psychologist and we did eye movement desensitisation and reprocessing therapy. It involves moving your eyes in a specific way while processing traumatic memories.” It also helped that Matthew was accompanying Sarah. “She actually said that she wanted to die in surgery,” he says, laughing. “She came out disappointed that she had not died.”
When Sarah developed depression, her family took her to a general physician. “I was given access to medication and psychological support quite early on,” she says. But, in high school, she hid her condition fearing stigma. Even into her late 20s, she did not show that she was struggling. She became a lot more open about it in her early 30s. “Because it was not easy to hide it when you are at the hospital (her workplace) or late for work, people know” she says. “In the past 10 years, I have lost all my inhibitions regarding talking about my depression and I have been really open about it with everyone. Because I know that if nobody is going to talk about it, [it would not be discussed enough]. So, we need to be more open about it.”
 Remote that controls the pulses emitted.
Remote that controls the pulses emitted.
Matthew, who works in the area of public health, says that Sarah's friends and colleagues found it difficult to understand her. He cannot recall the last time he saw her normal and well. “I struggle to remember what she was like before she was unwell,” he says. “It has been 24 years. In this time, she has not been able to express her interests and her personality in the ways she might have wanted to. There was a period from the ages of 14 to 18 where my parents, my brother and I noticed that she had less energy. She had several tests to check if there was some viral or post-viral fatigue or chronic fatigue problem, hormonal disturbance, because we did not know that there was all this stuff inside her. She was not telling anyone.” One of Sarah's friends, too, had severe depression and had taken his life, says Matthew.
He says that when she first stopped going to work, the family thought it was stress. “She had been put in a stressful position and then several people had left the government department she was working with,” he says. “She kept getting promoted and given more and more work, and eventually she burnt out. Then, she was studying and the same thing happened. She became more and more stressed. It was the depression causing the stress.”
Despite being a family of doctors and PhDs, the Reeves family was helpless. “We felt angry and guilty that someone in our family had to go through this and we could not do anything,” he says. “If it was not for depression, Sarah would have been married a long time ago. Everyone else in our generation in the family has done studies to the level of a doctor or a PhD doctorate. But Sarah, who was academically bright, had her studies interrupted.”
Sarah lived in India for a while, working as an occupational therapist and would have loved to settle here as she was enjoying it. But it was not possible to maintain that for long because it was a stressful job. “Just like cancer, severe depression aims at every part of your life and removes all the potential and capability and opportunities,” says Matthew. “That was also our thinking and reasoning when it came to surgery for depression. When we can go for surgery for deadly cancer, then why not this? They are both life threatening.”

Nobody in the Reeves family has had severe depression similar to Sarah's. However, relatives on both her mother's and father's side have had depression that was manageable with medication.
The DBS surgery for depression is prohibited in Australia. Doshi says the surgery is not without risks. “There is 1-2 per cent risk of death, with bleeding,” he says. “It is low, but not insignificant. That is one of the reasons it is not approved in Australia.” Matthew says even a 50 per cent chance of death was worth it, in case Sarah was going to try to kill herself. “[Risk of] death in surgery is better than the risk of suicide attempt,” he says.
There are many Indians who want this surgery, but Doshi says the surgery cannot be offered to most Indian patients for multiple reasons. “Firstly, Indians with moderate to severe depression do not come with full medical history,” he says. “They do not fit into our selection criteria and one of the reasons is the lack of data. They have not been exposed to the proper level of treatment. It is critical that you exhaust all possible medical options and this is the final step.”
Doshi says that Indian patients mostly come in having tried haphazard treatment. “They say, 'I went for behavioural therapy, I did not like it, so I stopped',” he says. “They have no details, like date, prescription, psychiatrist's note or therapist's note, for us to know what the outcome and benefits were. Some say they tried more than 20 drugs, but cannot produce documentation. They do not even know the names of the drugs, the duration or who prescribed it.” Doshi said all this information is available in the case of international patients and that was why the surgery was being offered to international patients.
The preparation of the surgery begins one and a half months earlier. “After all approvals from the [authorities], we start preparing the patient 15 to 20 days before surgery and checking their medical fitness,” he says. “The patient is admitted two days prior to surgery and detailed investigation about the particular disease is made in an objective evaluation. There are a lot of video recordings and consultations with the patient and psychiatrist and we do objective scoring, which can tell us the exact status of the patient. A detailed description of the patient's symptoms is also captured.”
This is followed by an MRI under general anaesthesia, because the patient is required to remain still. The MRI is a long process of around 40 minutes for DBS patients as against 20 minutes for others. Then there is planning―where to go in the brain and how to go, counselling the patient (the patient is awake in most of these surgeries). The procedure involves making small holes on the head and inserting the electrodes.
“Once we insert the electrode, we stimulate the target and identify the response,” says Doshi. “In Sarah's case, her anxiety became better and she felt like connecting to her surroundings. Sarah said her fatigue was going away and that she was feeling more energetic―all this on the table. She said her anxiety was going away, but not sadness. Sadness takes a long time to go. But this told us that we are at the right spot and then we fixed the electrodes there, and then from behind the ears, connected the pacemaker, which is implanted under the chest.”
The target for the procedure is an area in the brain called Brodmann Area 25. “Everything is adjustable, programmable with a remote control that can be used by the patient and only the pacemakers are removable, not the electrodes,” says Doshi. In the case of Sarah, he says, she has covered most of the ground with regard to healing. “I do not think more healing is required,” he says. “She has reached 80 per cent normalcy and the last 15 to 20 per cent will come over a period of time.”